Blue Cross Blue Shield Appeal Form Texas
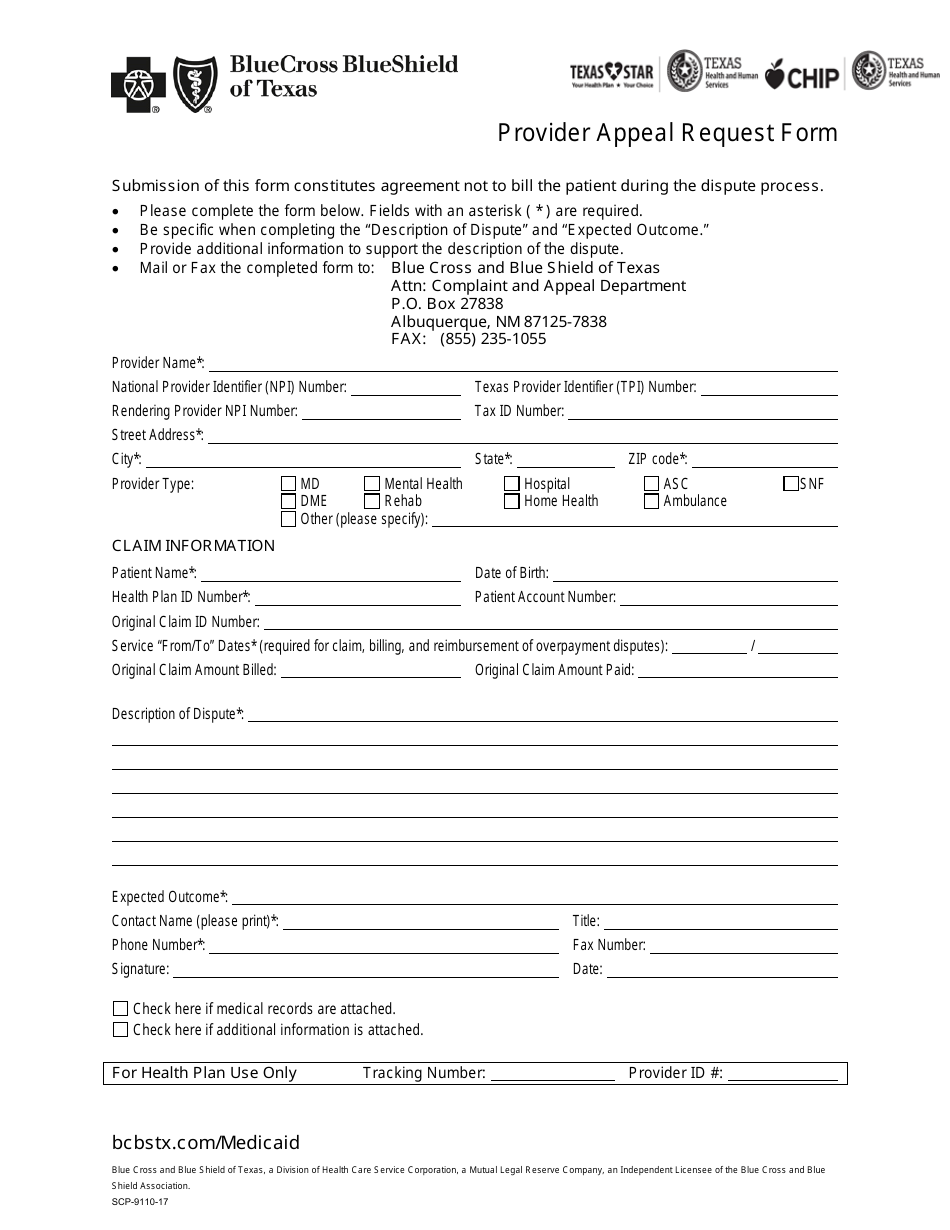
Blue Cross Blue Shield Appeal Form Texas - • please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Use the “claim appeal form” select only one reason for this request. • fields with an asterisk (*) are required. Do not use this form to request an appeal. Please fill out this form and attach any papers that support this request. • specify the “reason for claim. Facility/ancillary request for claim appeal/reconsideration review” form on top.
Do not use this form to request an appeal. Please fill out this form and attach any papers that support this request. • fields with an asterisk (*) are required. Facility/ancillary request for claim appeal/reconsideration review” form on top. • please complete one form per member to request an appeal of an adjudicated/paid claim. Use the “claim appeal form” select only one reason for this request. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. • specify the “reason for claim.
Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. • fields with an asterisk (*) are required. • please complete one form per member to request an appeal of an adjudicated/paid claim. Please fill out this form and attach any papers that support this request. Facility/ancillary request for claim appeal/reconsideration review” form on top. Use the “claim appeal form” select only one reason for this request. Do not use this form to request an appeal. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. • specify the “reason for claim.

Blue Cross Blue Shield of NC HQ Davis Kane
• please complete one form per member to request an appeal of an adjudicated/paid claim. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Use the “claim appeal form” select.
Blue Cross and Blue Shield of Texas Offering Medicare Advantage Plans
Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. • specify the “reason for claim. Please fill out this form and attach any papers that support this request. Do not use this form to request an appeal. Use the “claim appeal form” select only one reason for this request.
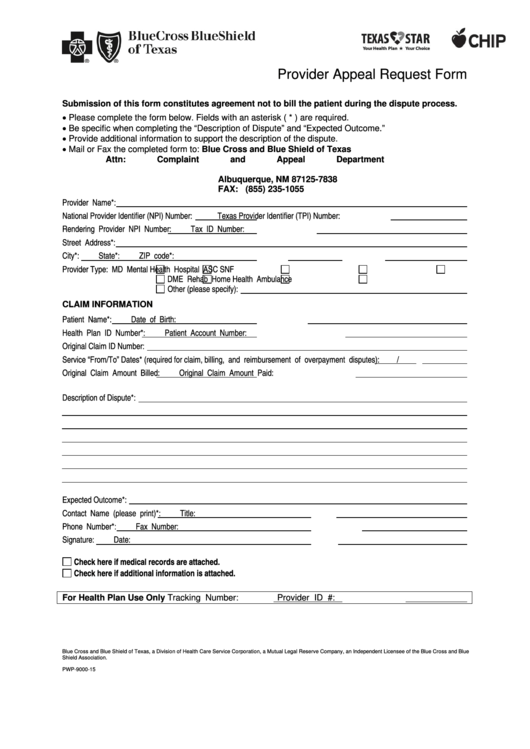
Form SCP911017 Fill Out, Sign Online and Download Printable PDF
• please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Facility/ancillary request for claim appeal/reconsideration review”.
Blue Cross Blue Shield Logo, symbol, meaning, history, PNG, brand
• fields with an asterisk (*) are required. Facility/ancillary request for claim appeal/reconsideration review” form on top. • please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Do not use this form to request an.

Blue cross blue shield overseas claim form Fill out & sign online DocHub
• specify the “reason for claim. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. • fields with an asterisk (*) are required. Do not use this form to request an appeal. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance.

Blue Cross and Blue Shield of Texas YouTube
Please fill out this form and attach any papers that support this request. Do not use this form to request an appeal. Use the “claim appeal form” select only one reason for this request. • specify the “reason for claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need.

Blue Cross Blue Shield Of Massachusetts Prior Authorization Form
Please fill out this form and attach any papers that support this request. Facility/ancillary request for claim appeal/reconsideration review” form on top. Use the “claim appeal form” select only one reason for this request. • fields with an asterisk (*) are required. Do not use this form to request an appeal.
Alignment Health Plan Provider Appeal Form
Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Facility/ancillary request for claim appeal/reconsideration review” form on top. • fields with an asterisk (*) are required. • specify the “reason for claim. Use the “claim appeal form” select only one reason for this request.
Capital Blue Cross Provider Appeal PDF Form FormsPal
• specify the “reason for claim. Use the “claim appeal form” select only one reason for this request. • please complete one form per member to request an appeal of an adjudicated/paid claim. Do not use this form to request an appeal. Facility/ancillary request for claim appeal/reconsideration review” form on top.

Rehabs that Accept Blue Cross Blue Shield Texas 24/7 Help
Please fill out this form and attach any papers that support this request. Do not use this form to request an appeal. Provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. Facility/ancillary request for claim appeal/reconsideration review” form on top. • fields with an asterisk (*) are required.
Please Fill Out This Form And Attach Any Papers That Support This Request.
• specify the “reason for claim. Blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Do not use this form to request an appeal. Facility/ancillary request for claim appeal/reconsideration review” form on top.
Provider Appeal Request Form • Please Complete One Form Per Member To Request An Appeal Of An Adjudicated/Paid Claim.
• fields with an asterisk (*) are required. • please complete one form per member to request an appeal of an adjudicated/paid claim. Use the “claim appeal form” select only one reason for this request.