Dental Health History Form Pdf
Dental Health History Form Pdf - If yes, what was the illness or problem? 3 history of infective endocarditis 4 artificial heart valve, repaired heart defect (pfo) 5 pacemaker or implantable defibrillator 6 congenital heart defect. Have you had a serious/difficult problem associated with any previous dental treatment? When was the last time your teeth were cleaned at a dental office? Are you taking or have you. How long has it been since your last dental visit? I will not hold my dentist or any member of his/her staff responsible for any. Are you having any problems now? Have you had a serious illness, operation or been hospitalized in the past 5 years? How often do you use dental floss?
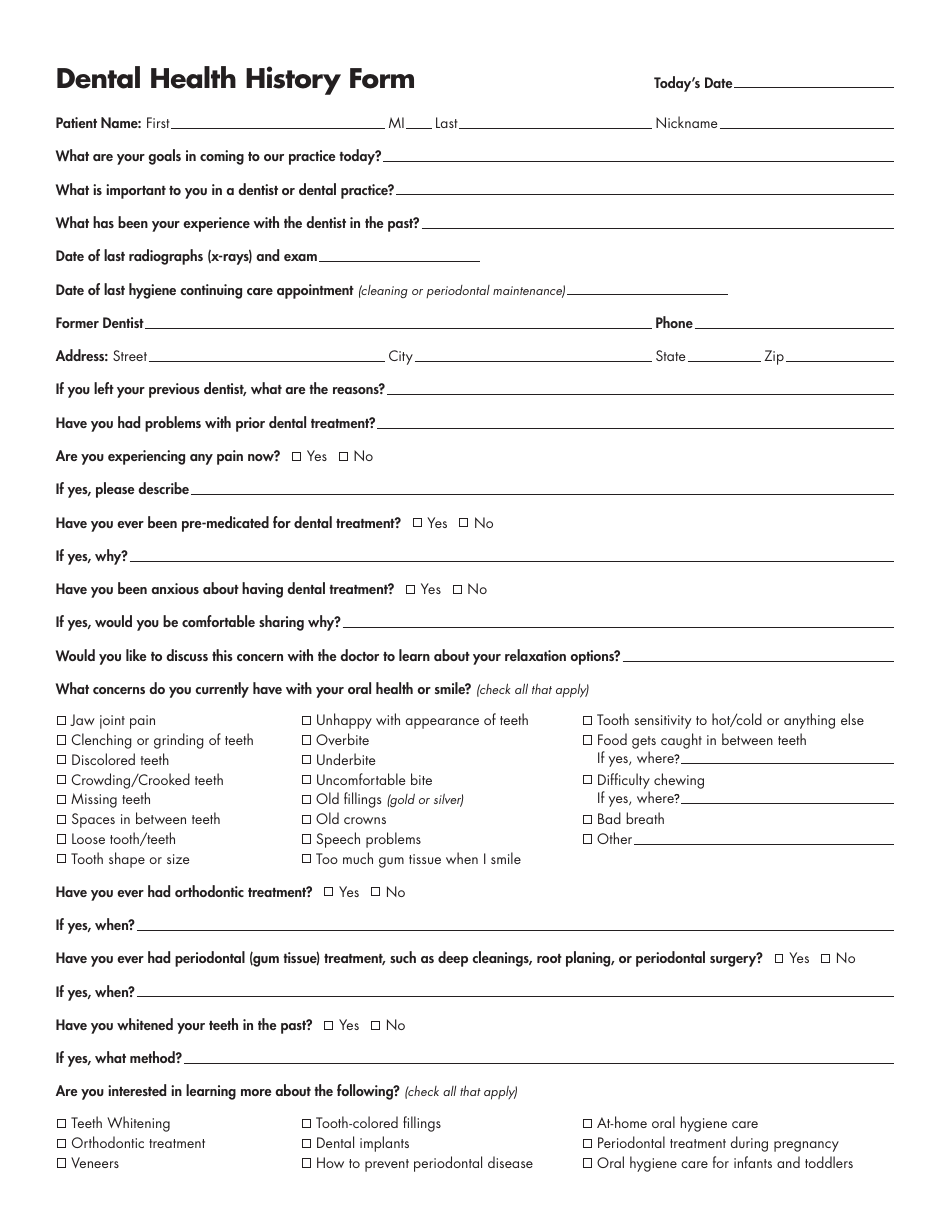
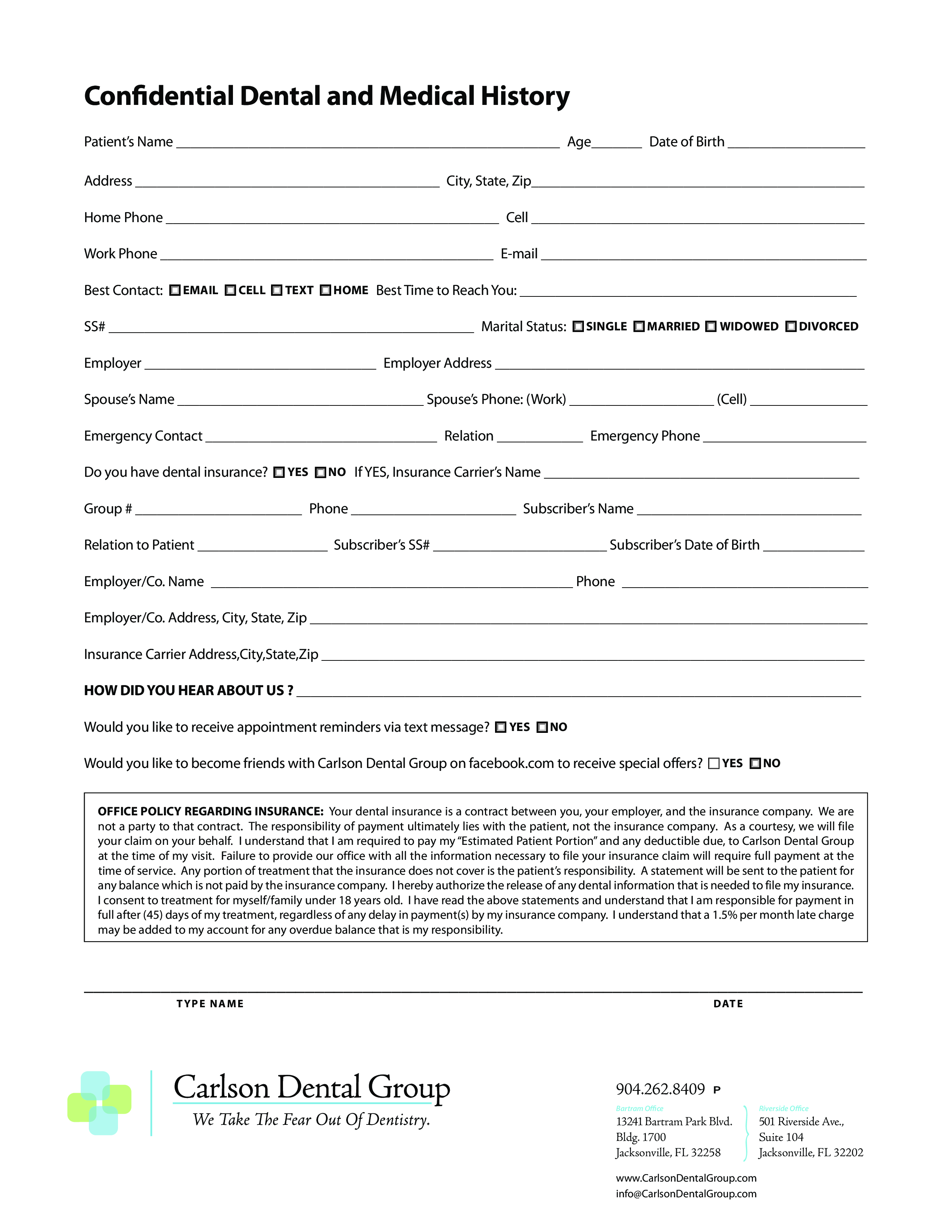
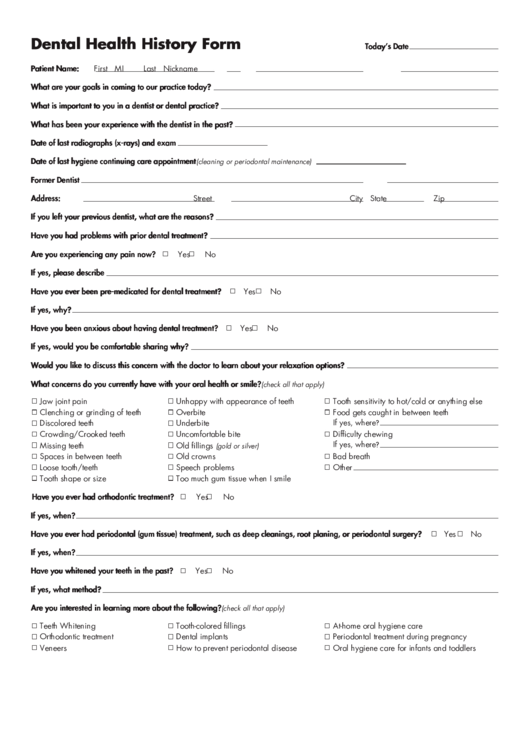
Fill out your personal and medical information,. Have you had a serious illness, operation or been hospitalized in the past 5 years? How would you describe your current dental problem? Are you taking or have you. 3 history of infective endocarditis 4 artificial heart valve, repaired heart defect (pfo) 5 pacemaker or implantable defibrillator 6 congenital heart defect. How long has it been since your last dental visit? I will not hold my dentist or any member of his/her staff responsible for any. If yes, what was the illness or problem? The above information is accurate and complete to the best of my knowledge. How often do you brush?
Fill out your personal and medical information,. How would you describe your current dental problem? How long has it been since your last dental visit? I will not hold my dentist or any member of his/her staff responsible for any. How often do you use dental floss? 3 history of infective endocarditis 4 artificial heart valve, repaired heart defect (pfo) 5 pacemaker or implantable defibrillator 6 congenital heart defect. Are you taking or have you. How often do you brush? If yes, what was the illness or problem? Download a pdf of the american dental association's health history form for dental patients.
Dental Health History Form Fill Out, Sign Online and Download PDF
Have you had a serious illness, operation or been hospitalized in the past 5 years? When was the last time your teeth were cleaned at a dental office? Fill out your personal and medical information,. I will not hold my dentist or any member of his/her staff responsible for any. How often do you brush?
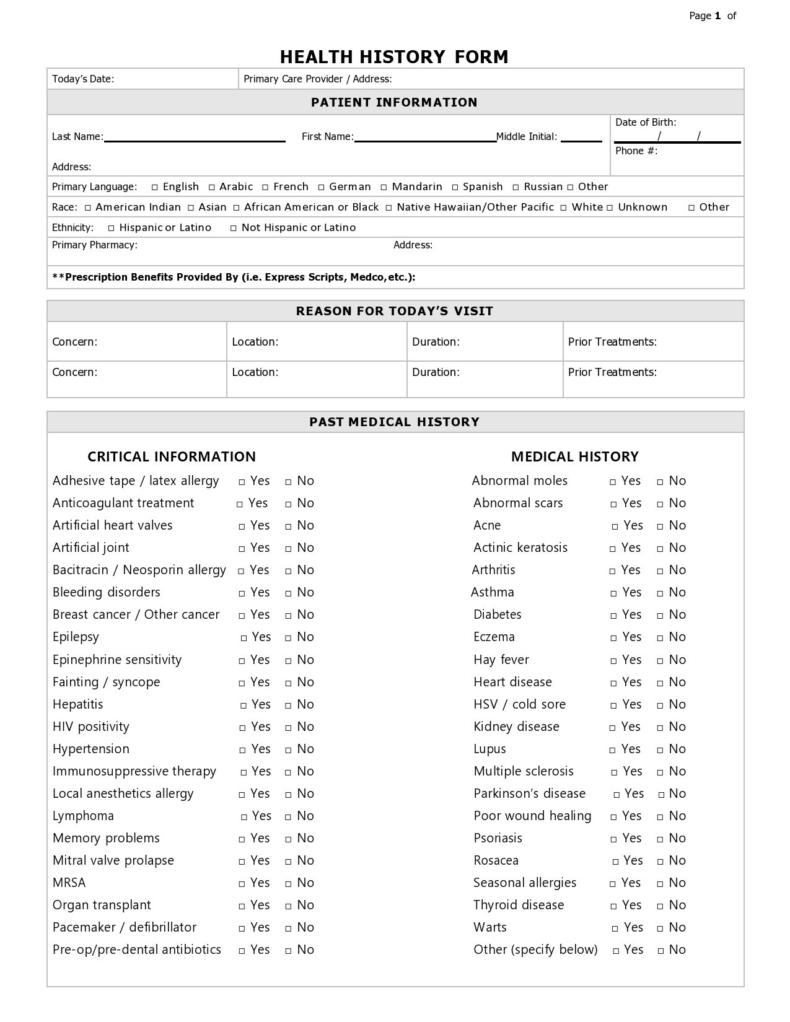
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-03-scaled-e1617709269345.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Fill out your personal and medical information,. Have you had a serious/difficult problem associated with any previous dental treatment? How often do you use dental floss? How would you describe your current dental problem? Download a pdf of the american dental association's health history form for dental patients.

Printable Medical History Form For Dental Office Printable Word Searches
I will not hold my dentist or any member of his/her staff responsible for any. Download a pdf of the american dental association's health history form for dental patients. Have you had a serious illness, operation or been hospitalized in the past 5 years? Fill out your personal and medical information,. Are you having any problems now?
Printable Dental Medical History Form Template Printable Templates
The above information is accurate and complete to the best of my knowledge. Download a pdf of the american dental association's health history form for dental patients. How often do you use dental floss? How often do you brush? Have you had a serious/difficult problem associated with any previous dental treatment?

Printable Medical History Form For Dental Office Printable Word Searches
How often do you use dental floss? Download a pdf of the american dental association's health history form for dental patients. How long has it been since your last dental visit? The above information is accurate and complete to the best of my knowledge. Are you having any problems now?
Medical History Form For Dental Office templates free printable
How would you describe your current dental problem? The above information is accurate and complete to the best of my knowledge. How long has it been since your last dental visit? Are you taking or have you. Fill out your personal and medical information,.
Dental Health History Form printable pdf download
Have you had a serious illness, operation or been hospitalized in the past 5 years? I will not hold my dentist or any member of his/her staff responsible for any. How often do you brush? If yes, what was the illness or problem? Have you had a serious/difficult problem associated with any previous dental treatment?
Printable Medical History Form
Fill out your personal and medical information,. Are you taking or have you. Download a pdf of the american dental association's health history form for dental patients. Are you having any problems now? Have you had a serious/difficult problem associated with any previous dental treatment?

Dental Health History Form Template
I will not hold my dentist or any member of his/her staff responsible for any. Fill out your personal and medical information,. Download a pdf of the american dental association's health history form for dental patients. Are you having any problems now? How would you describe your current dental problem?
Printable Dental Medical History Form Template Printable Templates
Download a pdf of the american dental association's health history form for dental patients. 3 history of infective endocarditis 4 artificial heart valve, repaired heart defect (pfo) 5 pacemaker or implantable defibrillator 6 congenital heart defect. Fill out your personal and medical information,. How would you describe your current dental problem? The above information is accurate and complete to the.
Have You Had A Serious/Difficult Problem Associated With Any Previous Dental Treatment?
How long has it been since your last dental visit? 3 history of infective endocarditis 4 artificial heart valve, repaired heart defect (pfo) 5 pacemaker or implantable defibrillator 6 congenital heart defect. Are you having any problems now? Download a pdf of the american dental association's health history form for dental patients.
How Would You Describe Your Current Dental Problem?
When was the last time your teeth were cleaned at a dental office? Are you taking or have you. Have you had a serious illness, operation or been hospitalized in the past 5 years? How often do you use dental floss?
How Often Do You Brush?
If yes, what was the illness or problem? Fill out your personal and medical information,. I will not hold my dentist or any member of his/her staff responsible for any. The above information is accurate and complete to the best of my knowledge.