Formexpress Scripts Appeal Form Non Medicare
Formexpress Scripts Appeal Form Non Medicare - Request for restriction on use and disclosure of health care information and/or. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Expedited appeal requests can be made by phone at. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. If you would like to request a coverage determination (such as an exception to the rules or restriction on our.
Expedited appeal requests can be made by phone at. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Request for restriction on use and disclosure of health care information and/or. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision.
If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Request for restriction on use and disclosure of health care information and/or. If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Expedited appeal requests can be made by phone at.
Fillable Express Scripts Claim Form printable pdf download
If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Request for restriction on use and disclosure of health care information and/or. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If your request for prescription coverage was denied, you have.

Fillable Online Express Scripts Claim Form. Claim form written by
Expedited appeal requests can be made by phone at. If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Request for restriction on use and disclosure of health care information and/or. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If.
Notice Of Medicare Non Coverage Form 2020 Form Resume Examples
Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Expedited appeal requests can be made by phone at. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. If you would like to request a coverage determination (such as an.
Anthem Provider Dispute Resolution 20092025 Form Fill Out and Sign
Expedited appeal requests can be made by phone at. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. If you would like to request a coverage determination (such as an.
Fillable Medicare Advantage Request Form For Appeal Wellmark
Request for restriction on use and disclosure of health care information and/or. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If you would like to request a coverage determination.
Medicare Irmaa 2024 Appeal Form Pdf Sella Daniella
Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Expedited appeal requests can be made by phone at. Request for restriction on use and disclosure of health care information and/or. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision..
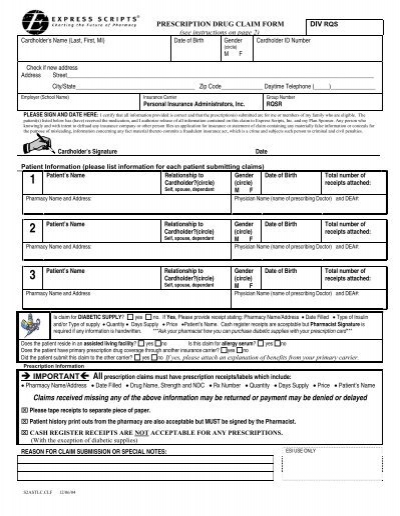
Claim Form for Express Scripts Prescriptions
Expedited appeal requests can be made by phone at. If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If your request for prescription coverage was denied, you have the right to.

Express Scripts Prior Authorization Form Printable
If you would like to request a coverage determination (such as an exception to the rules or restriction on our. Request for restriction on use and disclosure of health care information and/or. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Expedited appeal requests can be made by.
Medicare Open Enrollment Pharmacy Benefit Plans Express Scripts Fill
Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Expedited appeal requests can be made by phone at. Request for restriction on use and disclosure of health care information and/or. If you would like to request a coverage determination (such as an exception to the rules or restriction on our. If.

Medicare Appeal Form Cms20027 Medicare (United States) Medicaid
If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Request for restriction on use and disclosure of health care information and/or. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Expedited appeal requests can be made by phone at..
Expedited Appeal Requests Can Be Made By Phone At.
If you would like to request a coverage determination (such as an exception to the rules or restriction on our. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Request for restriction on use and disclosure of health care information and/or.