Free Medical Clearance Form For Dental
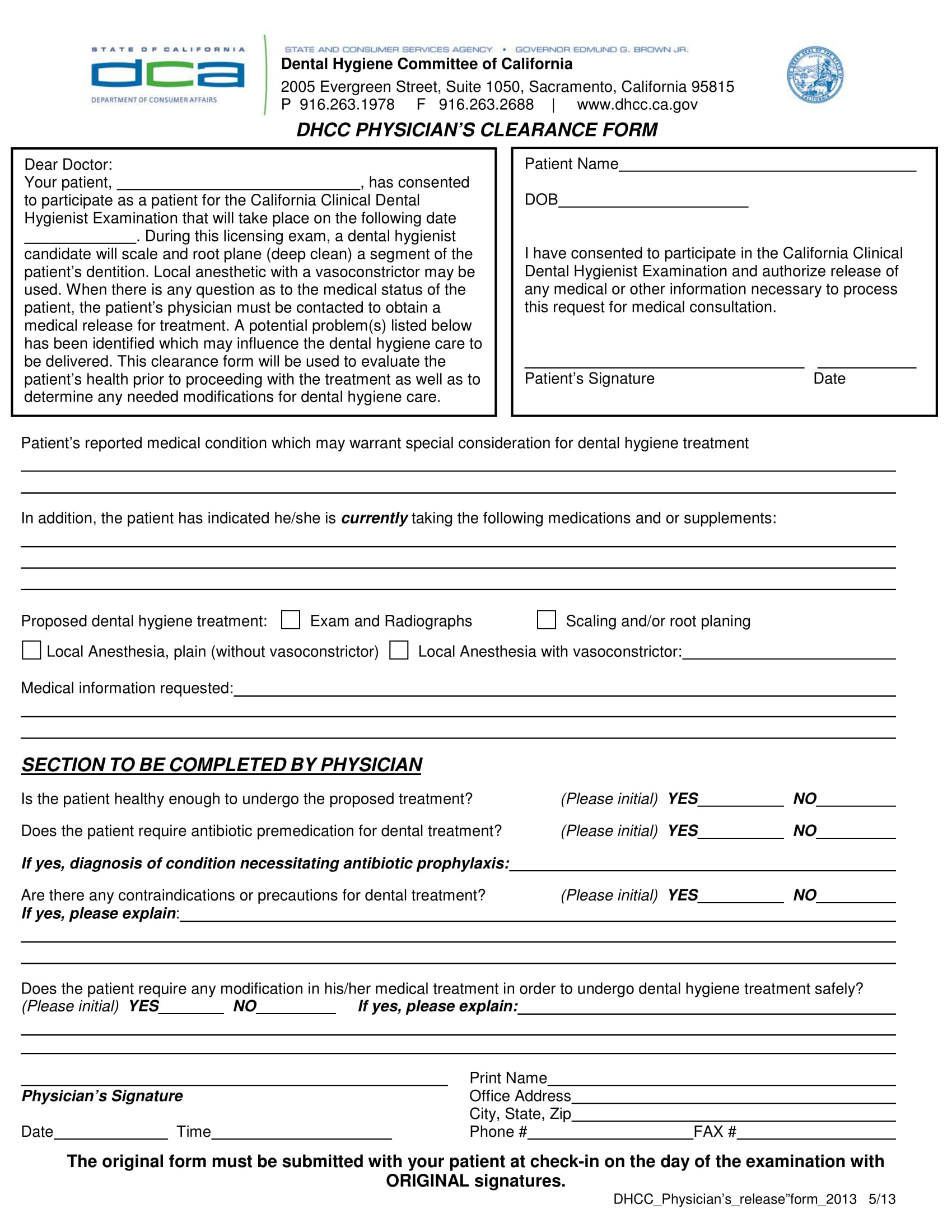
Free Medical Clearance Form For Dental - Medical clearance for dental treatment form. We appreciate your assistance in providing optimum care for this patient. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance form patient’s name: This document is essential for obtaining medical clearance prior to dental procedures.
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance form patient’s name: Medical clearance for dental treatment form. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. This document is essential for obtaining medical clearance prior to dental procedures. We appreciate your assistance in providing optimum care for this patient.
We appreciate your assistance in providing optimum care for this patient. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance form patient’s name: This document is essential for obtaining medical clearance prior to dental procedures. Medical clearance for dental treatment form.

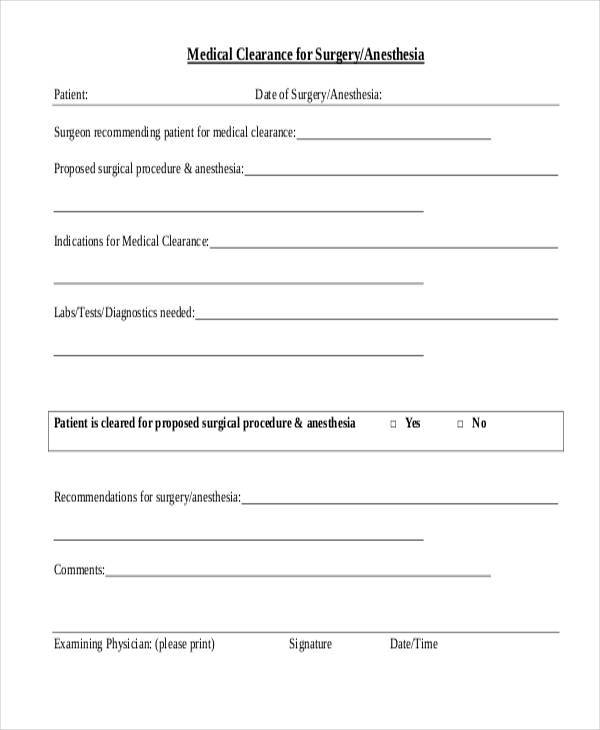
Printable Dental Clearance Form For Surgery Printable Word Searches
Medical clearance for dental treatment form. This document is essential for obtaining medical clearance prior to dental procedures. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. We appreciate your assistance in providing.
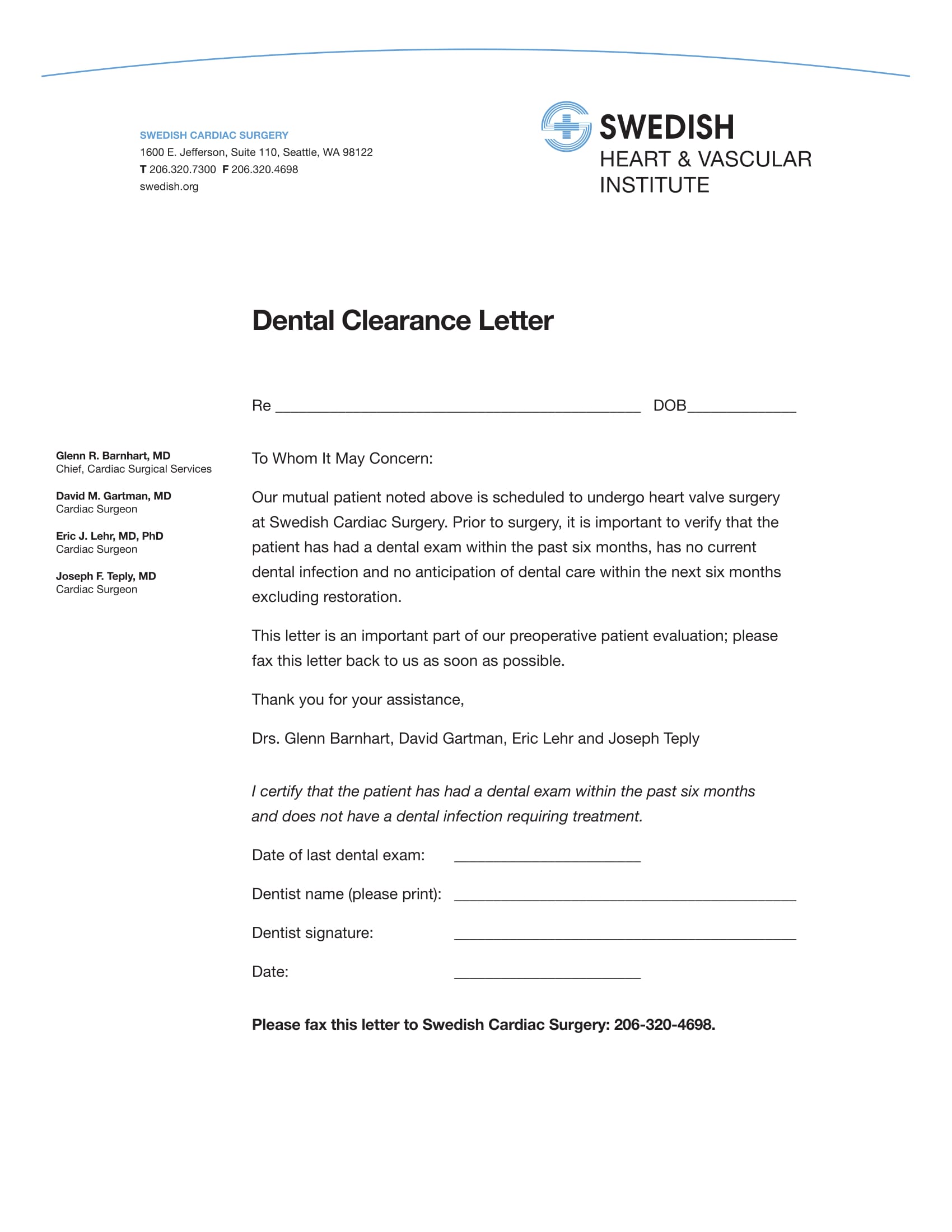
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. We appreciate your assistance in providing optimum care for this patient. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance form patient’s name: Medical clearance for dental treatment form.

Printable Dental Clearance Form
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance for dental treatment form. Medical clearance form patient’s name: This document is essential for obtaining medical clearance prior to dental procedures.
Dental Medical Clearance Form Printable Printable Word Searches
We appreciate your assistance in providing optimum care for this patient. This document is essential for obtaining medical clearance prior to dental procedures. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance form patient’s name: Medical clearance for dental treatment form.
Printable Dental Clearance Form For Surgery
Medical clearance form patient’s name: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. We appreciate your assistance in providing optimum care for this patient. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance for dental treatment form.
Printable Dental Clearance Form Printable Word Searches
Medical clearance for dental treatment form. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. This document is essential for obtaining medical clearance prior to dental procedures. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance form patient’s name:

Printable Medical Clearance Form For Dental Treatment
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. This document is essential for obtaining medical clearance prior to dental procedures. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance form patient’s name: Medical clearance for dental treatment form.
Printable Medical Clearance Form For Dental Printable Forms Free Online
This document is essential for obtaining medical clearance prior to dental procedures. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. _____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance form patient’s name: Medical clearance for dental treatment form.
Sample Medical Clearance Forms (Dental, Surgery, Work, etc.)
Medical clearance form patient’s name: This document is essential for obtaining medical clearance prior to dental procedures. We appreciate your assistance in providing optimum care for this patient. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. _____ dear doctor, our mutual patient has presented for dental treatment.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
_____ dear doctor, our mutual patient has presented for dental treatment with the following medical. Medical clearance form patient’s name: This document is essential for obtaining medical clearance prior to dental procedures. We appreciate your assistance in providing optimum care for this patient. Medical clearance for dental treatment form.
Please Ensure That Your Medical Provider Completes This Form And Returns It To Your Dental Office Before Your Scheduled Dental Procedure.
_____ dear doctor, our mutual patient has presented for dental treatment with the following medical. This document is essential for obtaining medical clearance prior to dental procedures. Medical clearance for dental treatment form. Medical clearance form patient’s name: