Sunshine Health Provider Appeal Form
Sunshine Health Provider Appeal Form - To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. The procedures for filing a complaint/grievance or. At sunshine health, both members and providers have the right to appeal decisions that affect their care and services. Download the provider claim adjustment request form (pdf). Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours.
Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. Download the provider claim adjustment request form (pdf). To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. The procedures for filing a complaint/grievance or. At sunshine health, both members and providers have the right to appeal decisions that affect their care and services. Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours.
Download the provider claim adjustment request form (pdf). At sunshine health, both members and providers have the right to appeal decisions that affect their care and services. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. The procedures for filing a complaint/grievance or. Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours. Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process.
Erisa Appeal 20162024 Form Fill Out and Sign Printable PDF Template
Download the provider claim adjustment request form (pdf). The procedures for filing a complaint/grievance or. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. At sunshine.
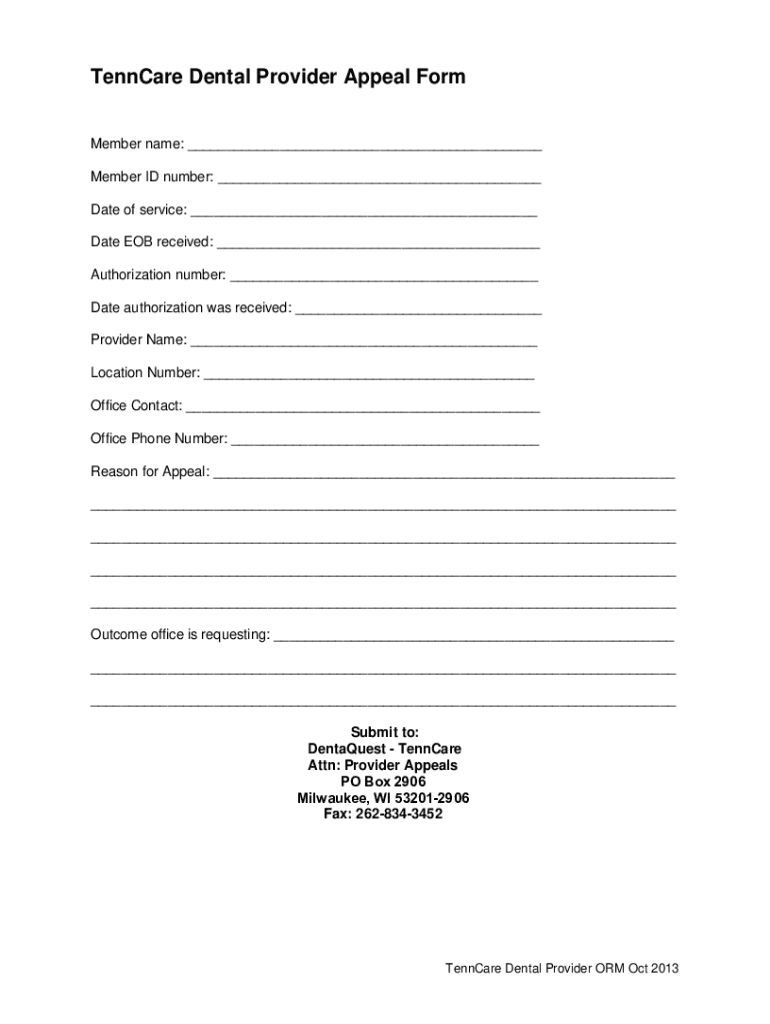
Fillable Online TennCare Dental Provider Appeal Form Fax Email Print
Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. The procedures for filing a complaint/grievance or. Providers may request an “expedited plan appeal”.
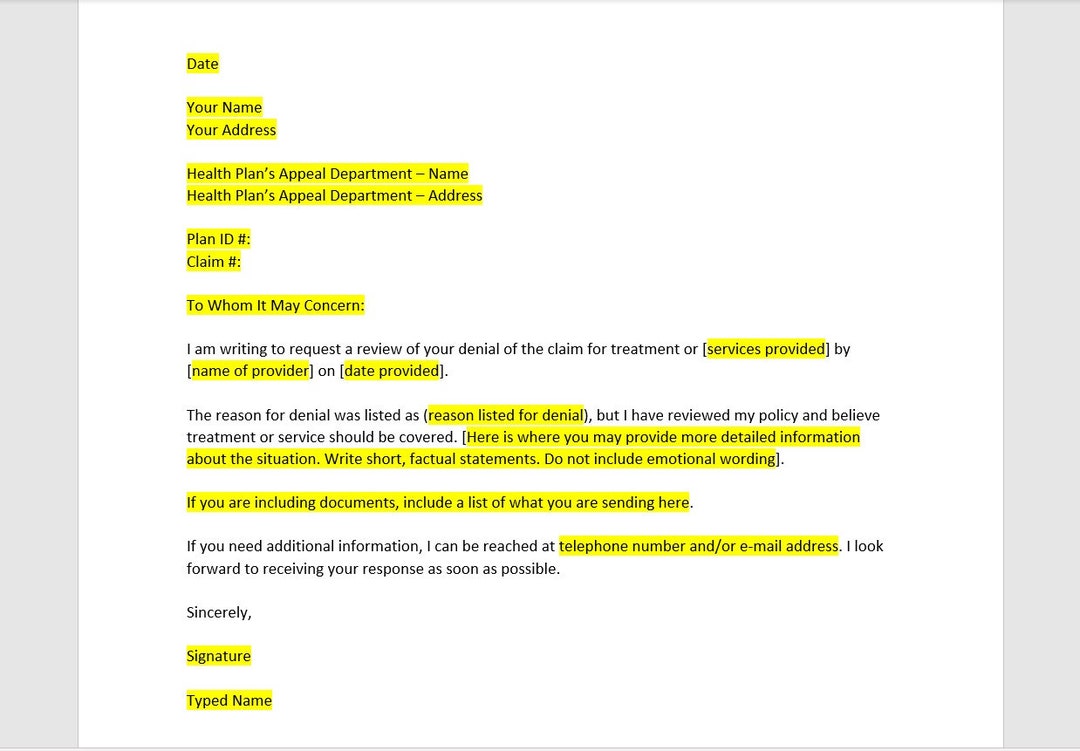
Health Insurance Appeal Letter Template, Health Insurance Appeal Letter
The procedures for filing a complaint/grievance or. To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Sunshine health must resolve the standard appeal within 30 days and an expedited.

Does Sunshine Health Cover Dermatologist
Download the provider claim adjustment request form (pdf). To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours. The procedures for filing a complaint/grievance or. Providers may request an “expedited plan appeal” on their.

Top United Healthcare Appeal Form Templates Free To Download In PDF
Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. The procedures for filing a complaint/grievance or. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. Download the provider claim adjustment request form (pdf). At sunshine.
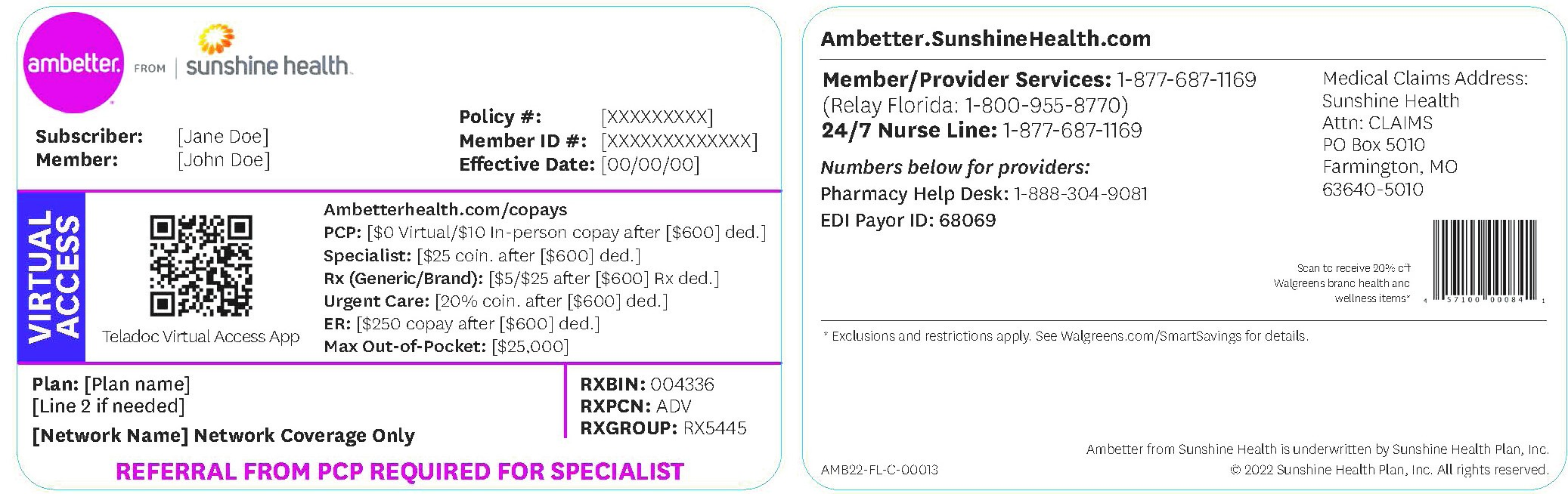
Provider Resources, Manuals & Forms Ambetter from Sunshine Health
Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection. Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. The procedures for filing a complaint/grievance or. Sunshine health must.

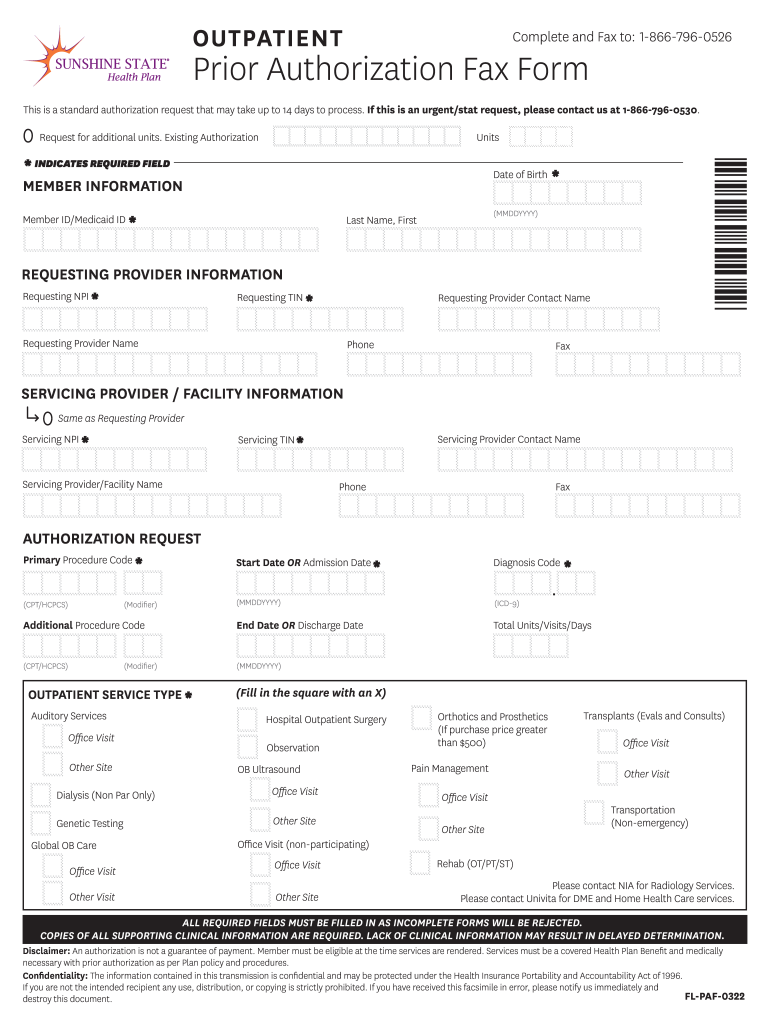
20212024 FL Sunshine State Health Plan Prior Authorization Fax Form
Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours. At sunshine health, both members and providers have.
Sunshine Authorization Form Edit & Share airSlate SignNow
At sunshine health, both members and providers have the right to appeal decisions that affect their care and services. To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Download the provider claim adjustment request form (pdf). The procedures for filing a complaint/grievance or. Providers may request an “expedited plan appeal”.
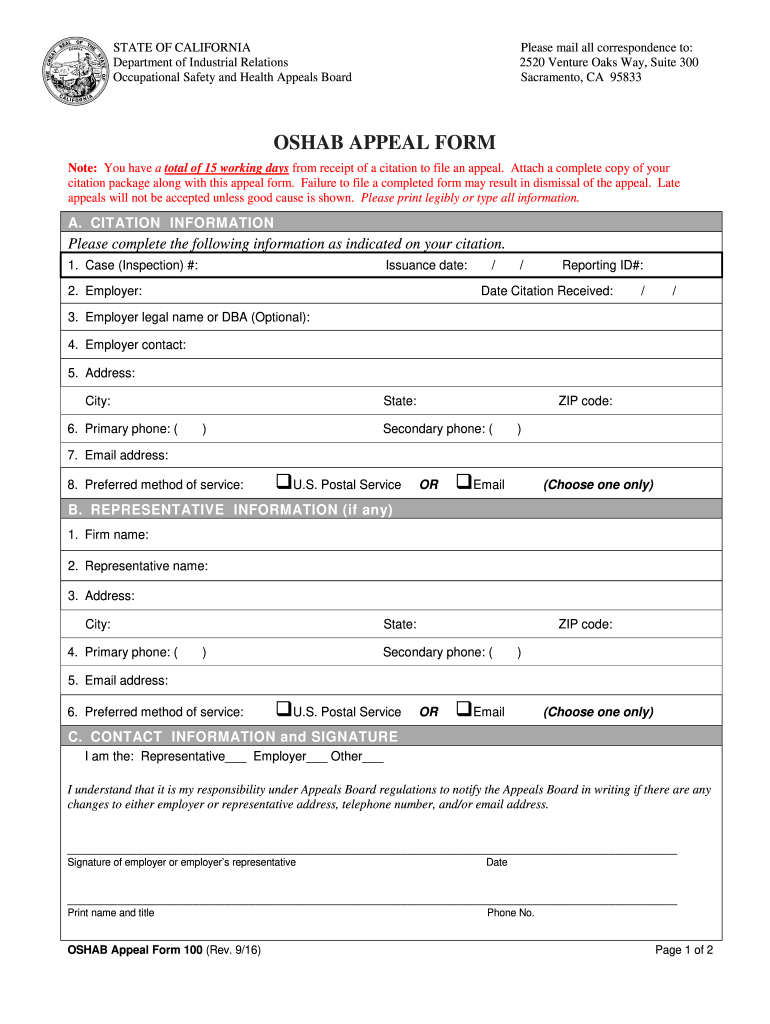
Health Plan Appeal Form ≡ Fill Out Printable PDF Forms Online
To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. The procedures for filing a complaint/grievance or. Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Providers may request an “expedited plan appeal” on their patients’ behalf if they.

Fill Free fillable Sunshine Health PDF forms
The procedures for filing a complaint/grievance or. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. Download the provider claim adjustment request form (pdf). Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Sunshine health must resolve the standard appeal within 30 days.
The Procedures For Filing A Complaint/Grievance Or.
Sunshine health must resolve the standard appeal within 30 days and an expedited appeal within 48 hours. To ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Providers may request an “expedited plan appeal” on their patients’ behalf if they believe. Any photocopied, black & white, or handwritten claim forms, regardless of the submission type (first time, corrected claim, request for reconsideration, or claim dispute) will cause an upfront rejection.
At Sunshine Health, Both Members And Providers Have The Right To Appeal Decisions That Affect Their Care And Services.
Use the provider claim adjustment request form to request adjustment of claim payment received that does not correspond with payment expected. Download the provider claim adjustment request form (pdf).