Uhc Appeal Form For Providers
Uhc Appeal Form For Providers - Learn how to appeal a coverage decision for a prescription drug under your medicare plan. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Find out how to file a grievance, appoint a.
Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Find out how to file a grievance, appoint a. Learn how to appeal a coverage decision for a prescription drug under your medicare plan.
Find out how to file a grievance, appoint a. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Learn how to appeal a coverage decision for a prescription drug under your medicare plan.
Uhc Designation Of Authorized Representative Form
Find out how to file a grievance, appoint a. Learn how to appeal a coverage decision for a prescription drug under your medicare plan. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is.
unitedhealthcare phone number
Learn how to appeal a coverage decision for a prescription drug under your medicare plan. Find out how to file a grievance, appoint a. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should.
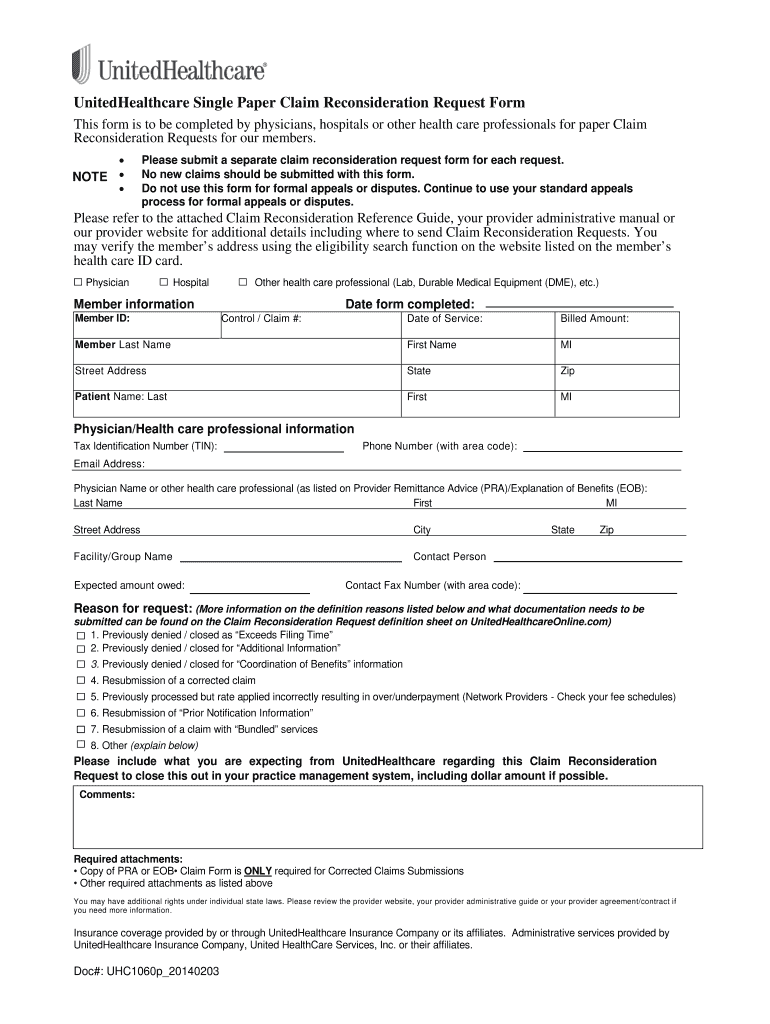
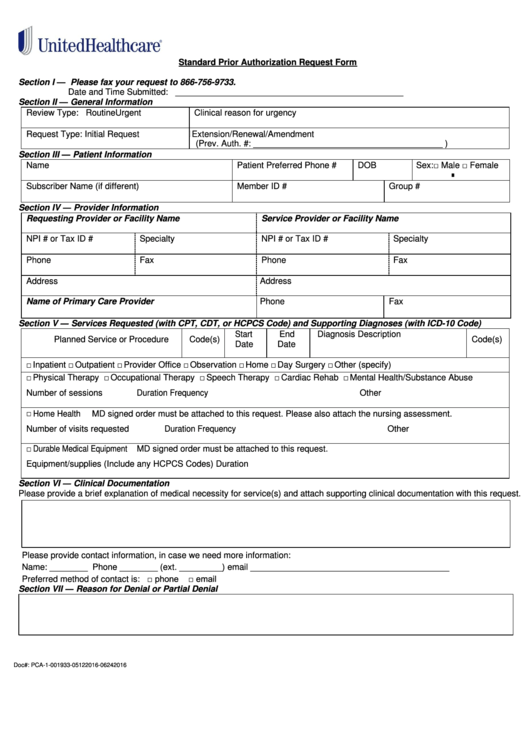
Uhc Reconsideration 20142024 Form Fill Out and Sign Printable PDF
Learn how to appeal a coverage decision for a prescription drug under your medicare plan. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Find out how to file a grievance, appoint a. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should.
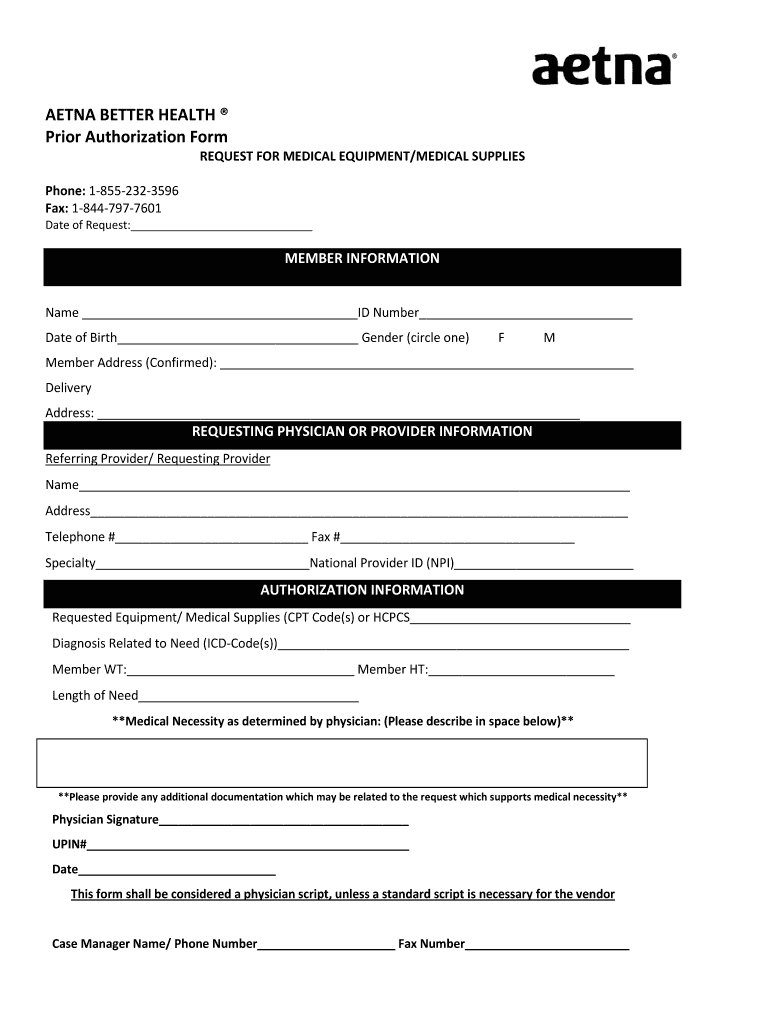
Aetna Better Health Prior Authorization Fill and Sign Printable
Learn how to appeal a coverage decision for a prescription drug under your medicare plan. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. Find out how to.
Aarp Provider Appeal Form Fill Online, Printable, Fillable, Blank
Find out how to file a grievance, appoint a. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Learn how to appeal a coverage decision for a prescription.

Uhc Appeal Form 2023 Printable Forms Free Online
To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Find out how to file a grievance, appoint a. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. Learn how to appeal a coverage decision for a prescription.
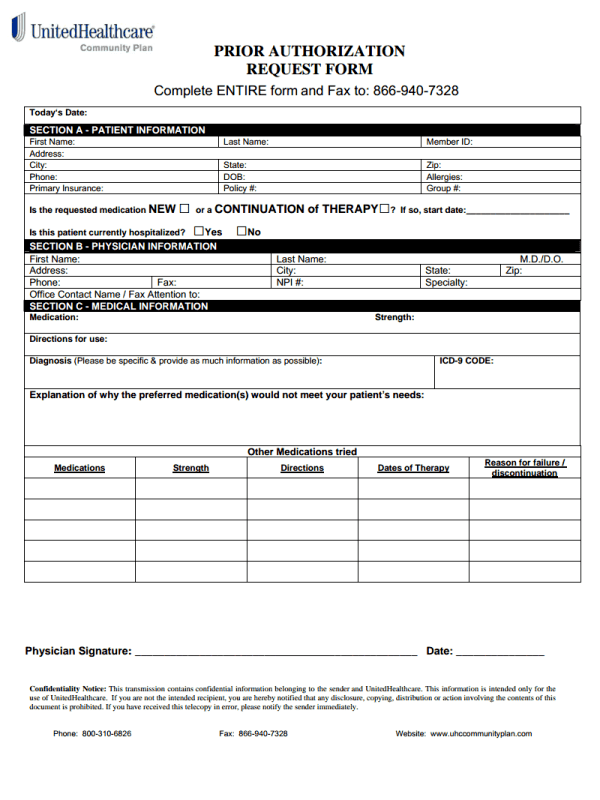
Authorization Fax Request Form Fill Online, Printable, Fillable
Find out how to file a grievance, appoint a. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. Learn how to appeal a coverage decision for a prescription drug under your medicare plan. To request reconsideration, health care professionals have 180 days from the date a claim is.

Valley Health Plan Appeal Form
To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. Find out how to file a grievance, appoint a. Learn how to appeal a coverage decision for a prescription.
unitedhealthcare phone number
Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. To request reconsideration, health care professionals have 180 days from the date a claim is denied in whole or partially. Learn how to appeal a coverage decision for a prescription drug under your medicare plan. Find out how to.
BCBS Provider Appeal Request Form Forms Docs 2023
Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for. Find out how to file a grievance, appoint a. Learn how to appeal a coverage decision for a prescription drug under your medicare plan. To request reconsideration, health care professionals have 180 days from the date a claim is.
To Request Reconsideration, Health Care Professionals Have 180 Days From The Date A Claim Is Denied In Whole Or Partially.
Find out how to file a grievance, appoint a. Learn how to appeal a coverage decision for a prescription drug under your medicare plan. Appeal requests must be submitted in writing and should clearly state “formal appeal request.” providers should state the specific reason for.